
Hypothyroidism Treatment: 8 Essential Levothyroxine Rules
Clinical Practice Update — Levothyroxine Dosing, Subclinical Thresholds, Pregnancy Adjustments, and Monitoring in Adults
This is an original clinical education article informed by current guidelines and evidence. See References below for source documents.
- Clinical Focus
- Evidence-based hypothyroidism treatment in adults across primary care and specialty settings
- Target Audience
- Primary care physicians, internists, endocrinologists, obstetricians, residents, pharmacists
- Setting
- Primary care, endocrinology clinic, antenatal care
- Source Evidence
- •ATA Guidelines for the Treatment of Hypothyroidism (Thyroid, 2014)
- •ATA Guidelines for Thyroid Disease in Pregnancy and Postpartum (2017)
- •ETA Guideline on Subclinical Hypothyroidism (Eur Thyroid J, 2013)
- •TRUST Trial — Levothyroxine in Older Adults with Subclinical Hypothyroidism (NEJM, 2017)
- •Feller et al. Meta-analysis on Thyroid Hormone and Quality of Life (JAMA, 2018)
Key Clinical Takeaways
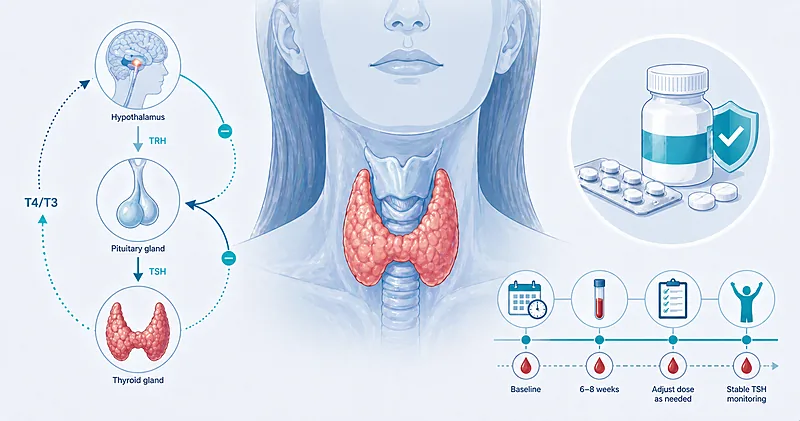
Effective hypothyroidism treatment is deceptively simple to get right: confirm the diagnosis biochemically, match the starting dose to age and cardiovascular risk, monitor TSH at the correct intervals, and adjust for life-stage changes such as pregnancy. The ATA framework gives clear thresholds for when to treat subclinical disease and when to defer. The points below translate the evidence into actionable rules.
- 1Prescribe levothyroxine monotherapy as the first-line agent for overt hypothyroidism — not T3 or desiccated thyroid → Initiation
- 2Start 1.6 µg/kg/day in healthy young adults; start 25–50 µg in patients over 60 or with coronary disease → Initiation
- 3Counsel patients to take levothyroxine on an empty stomach 30–60 minutes before food, or at bedtime 3+ hours after the last meal → Dosing Principles
- 4Treat subclinical hypothyroidism when TSH is above 10 mIU/L; individualise below that threshold → Subclinical Thresholds
- 5Avoid routine treatment of mildly elevated TSH in adults over 70 — TRUST showed no symptom or functional benefit → Subclinical Thresholds
- 6Do not offer combination T4/T3 therapy routinely — reserve for carefully selected patients with persistent symptoms → Combination Therapy
- 7Increase the dose by 25–30% the moment pregnancy is confirmed and target TSH under 2.5 mIU/L in the first trimester → Pregnancy
- 8Recheck TSH 6–8 weeks after any dose change; annually once stable → Monitoring
- 9Separate levothyroxine from calcium, iron, PPIs, cholestyramine, and antacids by at least 4 hours → Interactions
- 10Keep the patient on the same manufacturer (brand or generic) at every refill to avoid TSH swings → Monitoring
Initiating Hypothyroidism Treatment
Appropriate hypothyroidism treatment begins with biochemical confirmation. An elevated TSH alone can be due to recent illness, diurnal variation, or assay interference; pair it with a free T4 before committing the patient to lifelong therapy. Starting dose is chosen by age, weight, cardiovascular status, and the severity of hypothyroidism.
Confirm overt hypothyroidism with an elevated TSH and a low free T4 measured on two occasions at least 4–8 weeks apart. A single borderline TSH is not enough to commit a patient to lifelong therapy.
Strong Rec High Evidence ATA 2014Check anti-TPO antibodies in newly diagnosed patients. A positive result establishes autoimmune etiology, predicts progression of subclinical disease, and has implications for fertility and pregnancy planning.
Moderate Rec Moderate Evidence ATA 2014Start levothyroxine 1.6 µg/kg/day (ideal body weight) in otherwise healthy adults under 60 with overt hypothyroidism. Typical starting doses are 100–125 µg daily.
Strong Rec High Evidence ATA 2014Start with a low dose of 25–50 µg daily in adults over 60, those with known coronary artery disease, or those with long-standing severe hypothyroidism. Titrate up by 12.5–25 µg every 4–6 weeks based on TSH.
Strong Rec Moderate Evidence ATA 2014Counsel patients to take levothyroxine on an empty stomach 30–60 minutes before breakfast, or alternatively at bedtime at least 3 hours after the last meal. Bedtime dosing is equally effective for patients who cannot consistently manage a morning fast.
Strong Rec High Evidence ATA 2014Starting Dose by Clinical Scenario
| Patient Scenario | Starting Dose | Titration Increment | TSH Target | Practical Tips |
|---|---|---|---|---|
| Healthy adult <60 | 1.6 µg/kg/day (typically 100–125 µg) | 12.5–25 µg every 6 weeks | 0.4–4.0 mIU/L | Full replacement from day 1 is usually safe |
| Adult ≥60 or comorbid | 25–50 µg daily | 12.5–25 µg every 4–6 weeks | 1.0–4.0 mIU/L (less aggressive) | Watch for angina, arrhythmia during titration |
| Known coronary artery disease | 12.5–25 µg daily | 12.5 µg every 6–8 weeks | Symptom-guided | Coordinate with cardiology; may need partial replacement only |
| Severe long-standing hypothyroidism | 25–50 µg daily | 25 µg every 4–6 weeks | 0.4–4.0 mIU/L | Exclude adrenal insufficiency first |
| Post-thyroidectomy (benign) | 1.6 µg/kg/day | 25 µg every 6 weeks | 0.4–4.0 mIU/L | Start immediately postop in total thyroidectomy |
| Pregnancy (confirmed) | Increase existing dose by 25–30% | Adjust by TSH every 4 weeks | <2.5 mIU/L (T1); <3.0 (T2/T3) | Two extra tablets per week is a pragmatic shortcut |
Subclinical Hypothyroidism Treatment Thresholds
Subclinical hypothyroidism treatment is one of the most over-applied interventions in primary care. Thresholds exist for a reason: evidence for benefit below a TSH of 10 mIU/L is weak, and evidence for benefit in older adults is essentially absent. The TRUST trial and the 2018 Feller meta-analysis, together involving thousands of patients, found no quality-of-life improvement from levothyroxine in this group.
Treat subclinical hypothyroidism with a confirmed TSH above 10 mIU/L regardless of symptoms. Mortality and cardiovascular risk rise above this threshold in most observational datasets.
Strong Rec Moderate Evidence ATA 2014 ETA 2013Consider hypothyroidism treatment with TSH between 4.5 and 10 mIU/L only when the patient is under 70, has bothersome hypothyroid symptoms, is pregnant or planning pregnancy, has positive anti-TPO antibodies, or has significant cardiovascular risk.
Conditional Rec Moderate Evidence ETA 2013 ATA 2014Do not routinely initiate levothyroxine in adults over 70 with TSH between 4.5 and 10 mIU/L. Observe with repeat testing at 6 months; most TSH values in this range normalise spontaneously or remain stable without symptoms.
Against High Evidence TRUST 2017 Feller 2018Before labelling a raised TSH as subclinical hypothyroidism, exclude recovery from recent illness (non-thyroidal illness syndrome), heterophile antibody interference, and laboratory variability. Repeat the TSH with free T4 after 6–8 weeks before deciding.
Strong Rec Moderate Evidence ATA 2014Combination T4/T3 Therapy and Alternatives
Roughly 10–15% of patients on adequate levothyroxine therapy report persistent symptoms despite normal TSH. Whether this reflects imperfect tissue conversion of T4 to T3 in selected patients, or a non-thyroid explanation, remains debated. ATA and ETA both urge caution with T3-containing regimens and discourage desiccated thyroid extract.
Do not offer combination T4/T3 as first-line hypothyroidism treatment. Randomised trials have not shown consistent symptom or cognitive benefit over levothyroxine alone, and T3 has a short half-life that causes supraphysiologic peaks.
Against Moderate Evidence ATA 2014In patients with persistent symptoms on adequate levothyroxine and TSH in the low-normal range, consider a supervised trial of T4/T3 combination with liothyronine 5–10 µg daily, after non-thyroid causes have been excluded. Stop after 3–6 months if no benefit.
Conditional Rec Low Evidence ATA 2014 ETA 2012Do not prescribe desiccated thyroid extract (DTE) as routine hypothyroidism treatment. The T4:T3 ratio in DTE differs from human physiology, batch variability is substantial, and no well-designed trial has shown advantage over levothyroxine.
Against Low Evidence ATA 2014Pregnancy and Special Populations
Pregnancy doubles the thyroid hormone demand rapidly from the first trimester. Untreated maternal hypothyroidism is associated with miscarriage, preterm birth, and adverse neurodevelopmental outcomes. Every woman of reproductive age on levothyroxine needs a clear action plan for what happens when the pregnancy test turns positive.
Preconception, target TSH in the lower half of the reference range (typically <2.5 mIU/L) in any woman on levothyroxine who is planning pregnancy.
Strong Rec Moderate Evidence ATA 2017Increase the existing levothyroxine dose by 25–30% as soon as pregnancy is confirmed. A practical shortcut: take two extra tablets per week (9 tablets per week instead of 7).
Strong Rec High Evidence ATA 2017Target TSH below 2.5 mIU/L in the first trimester and below 3.0 mIU/L in the second and third trimesters. Check TSH every 4 weeks until 20 weeks, then at 24–28 and 32–34 weeks.
Strong Rec Moderate Evidence ATA 2017Return to the pre-pregnancy dose immediately after delivery and recheck TSH 6 weeks postpartum. Breastfeeding is compatible with levothyroxine therapy.
Strong Rec Moderate Evidence ATA 2017Screen women of reproductive age with a TSH when they present for infertility evaluation, recurrent miscarriage, or anti-TPO positivity. Treat overt hypothyroidism before conception wherever possible.
Strong Rec Moderate Evidence ATA 2017Clinical Decision Pathway
A practical, question-based approach to adult hypothyroidism treatment from the first abnormal TSH to long-term maintenance.
Monitoring and Drug Interactions
Many “refractory” hypothyroidism presentations are actually failures of absorption, interaction, or adherence. Systematic review of these variables at every visit prevents unnecessary dose escalation.
Common Drug and Food Interactions with Levothyroxine
| Interaction Category | Examples | Effect on Levothyroxine | Practical Management |
|---|---|---|---|
| Impaired absorption | Calcium, iron, cholestyramine, sucralfate, aluminium antacids, soy, fibre supplements | TSH rises despite stable dose | Separate doses by at least 4 hours |
| Proton pump inhibitors | Omeprazole, pantoprazole, esomeprazole | Modestly reduced absorption (gastric pH-dependent) | Liquid or soft-gel formulations less affected; recheck TSH after starting |
| Increased binding | Oestrogens (OCP, HRT), tamoxifen, pregnancy | Increased TBG → higher dose requirement | Check TSH 6–8 weeks after starting oestrogen |
| Accelerated metabolism | Rifampin, phenytoin, carbamazepine, phenobarbital | Faster clearance → higher dose need | Recheck TSH after starting or stopping |
| Decreased T4 to T3 conversion | Amiodarone, high-dose beta-blockers, severe illness | Altered free T4/T3 ratio | Interpret with clinical context; avoid routine dose changes |
| Food and coffee | Any breakfast, coffee within 30–60 min | Reduced bioavailability | Fasted morning dose or bedtime dose |
Monitoring Schedule
| Clinical Situation | When to Check TSH | Common Pitfalls |
|---|---|---|
| Initiation or dose change | 6–8 weeks after change | Checking at 2–3 weeks — TSH has not equilibrated |
| Stable patient | Annually | Excessive testing with no clinical trigger |
| Starting interacting medication | 6–8 weeks later | Missing the interaction and escalating dose without cause |
| Pregnancy | Every 4 weeks to 20 weeks, then 24–28 and 32–34 | Forgetting the return-to-baseline dose postpartum |
| Persistent symptoms, normal TSH | Consider free T4; screen non-thyroid causes | Escalating levothyroxine into thyrotoxic range |
Evidence in Context
What the major trials tell us, where the guidelines align, and where important questions remain.
Where ATA and ETA Agree
Both guideline bodies converge on levothyroxine as first-line monotherapy for overt hypothyroidism, treatment of TSH >10 mIU/L in most adults, a lower TSH target in pregnancy, and caution about T4/T3 combination therapy outside of selected patients. Both emphasise correct administration (fasting or bedtime) and the need to screen for interacting medications.
TRUST and the Older Adult Question
TRUST randomised 737 adults over 65 with subclinical hypothyroidism (TSH 4.6–20 mIU/L) to levothyroxine or placebo. After a median of one year, there was no meaningful improvement in hypothyroid symptoms, fatigue, cognition, activities of daily living, or quality of life, despite successful TSH normalisation in the treated group. The trial re-shaped guidance for older adults with mildly elevated TSH.
Feller Meta-Analysis: Looking Beyond TRUST
The 2018 JAMA meta-analysis pooled 21 randomised trials and over 2,000 adults with subclinical hypothyroidism. Thyroid hormone therapy did not significantly improve general quality of life or thyroid-related symptoms. The effect estimate crossed unity across almost every domain. The authors concluded that the evidence does not support broad treatment of subclinical hypothyroidism for symptom relief.
The T4/T3 Combination Debate
Multiple randomised trials of T4/T3 combination have produced conflicting results. Most failed to show improvement over T4 alone in the primary endpoints, though a minority of patients prefer combination therapy in blinded crossover designs. A genetic polymorphism in the deiodinase type 2 gene (DIO2) has been proposed as a modifier but is not yet validated for clinical use. The takeaway: T4 alone works for most; a supervised trial of combination therapy is reasonable for selected patients with persistent symptoms.
What We Still Don’t Know
Several important questions remain unresolved in hypothyroidism treatment. Whether treatment of subclinical disease in middle-aged adults prevents cardiovascular events has not been settled by a large trial. Whether biomarkers (DIO2 polymorphism, free T3 levels) can identify patients who benefit from combination therapy needs prospective validation. The optimal TSH target within the normal range — low-normal versus mid-normal — is also an open question.
References
- 1.Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement. Thyroid. 2014;24(12):1670–1751. doi:10.1089/thy.2014.0028
- 2.Alexander EK, Pearce EN, Brent GA, et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid. 2017;27(3):315–389. doi:10.1089/thy.2016.0457
- 3.Pearce SH, Brabant G, Duntas LH, et al. 2013 ETA Guideline: Management of Subclinical Hypothyroidism. Eur Thyroid J. 2013;2(4):215–228. doi:10.1159/000356507
- 4.Stott DJ, Rodondi N, Kearney PM, et al. Thyroid Hormone Therapy for Older Adults with Subclinical Hypothyroidism (TRUST). N Engl J Med. 2017;376(26):2534–2544. doi:10.1056/NEJMoa1603825
- 5.Feller M, Snel M, Moutzouri E, et al. Association of Thyroid Hormone Therapy With Quality of Life and Thyroid-Related Symptoms in Patients With Subclinical Hypothyroidism: A Systematic Review and Meta-analysis. JAMA. 2018;320(13):1349–1359. doi:10.1001/jama.2018.13770
- 6.Wiersinga WM, Duntas L, Fadeyev V, Nygaard B, Vanderpump MP. 2012 ETA Guidelines: The Use of L-T4 + L-T3 in the Treatment of Hypothyroidism. Eur Thyroid J. 2012;1(2):55–71. doi:10.1159/000339444
How to Read the Evidence Tags
Every recommendation carries two tags for strength and evidence quality, plus a source tag — Medaptly’s own simplified interpretations.
Recommendation Strength
| Tag | What It Means |
|---|---|
| Strong Rec | High-quality evidence broadly supports this action. |
| Moderate Rec | The weight of evidence favours this action. |
| Conditional Rec | The benefit is less certain — individualise. |
| Against | Evidence shows no benefit or potential harm. |
Evidence Quality
| Tag | What It Means |
|---|---|
| High Evidence | Multiple well-designed RCTs or high-quality meta-analyses. |
| Moderate Evidence | Single RCT or large observational studies. |
| Low Evidence | Expert consensus or small studies. |